

Copyright 2015 © Nigerian Journal of Paediatrics. All Rights Reserved. . Powered by Pelrox Technologies Ltd
ISSN 03 02 4660 AN OFFICIAL JOURNAL OF THE PAEDIATRIC ASSOCIATION OF NIGERIA

|










Quick Navigation

Niger J Paediatr 2016; 43 (2):102 103
LETTER TO THE EDITOR
DOI:http://dx.doi.org/10.4314/njp.v43i2.8
Accepted: 16th March 2016
Are we losing the gains of the Oral
Ekanem EE (
)
Akinwunmi F
Rehydration Therapy Strategy? An
Department of Paediatrics,
illustrative case
University of Calabar, Calabar,
Nigeria.
Community Health Department,
Shell Petroleum Development
Company of Nigeria
Email: emmanuel.ekanem@shell.
Dear Editor,
tube. PCV dropped to 21% by the sixth day and child
was transfused. Infant regained consciousness after
Incidence and deaths from diarrhoea in childhood have
seven days but with evidence of cortical damage- in-
declined remarkably in the last decade. Much of this
1
creased tone in all limbs and cortical blindness.
could be attributed to the Oral Rehydration Therapy
strategy introduced by the WHO . In Nigeria, this was
2
It
would appear we are beginning to lose some of the
adapted into standard guidelines with salutary effects .
3
gains made by the ORT strategy. In this illustrative case,
The strategy hinges on hygienic practices, non-use of
the mother, from a sub-urban area, was using feeding
feeding bottles, use of appropriate oral fluids for the
bottle to feed the infant. The ORS was improperly
prevention and correction of dehydration from diar-
mixed and may explain the hypernatraemia and subse-
rhoea, selective use of antimicrobials, continued feeding
quent convulsions and coma. Several branded drugs
during episodes of diarrhoea, avoidance of anti-emetics
containing promethiazine, chlorpheneramine, hyoscine
and anti-motility drugs . A recent study has demon-
2
bromide, pseudoephedrine, kaolin, some of which may
strated inappropriate use and abuse of anti-microbials,
have
contributed to the childs seizures and coma, were
anti-emetics and anti-motility drugs at all levels of the
given. In addition, several anti-microbials were given.
health system in Nigeria . At a Community Cottage
4
The sedation, which interfered with feeding, contributed
Hospital in the Niger Delta supported by Shell Petro-
to
the severe hypoglycaemia. The use and abuse of vari-
leum Development Company, children are often seen
ous oral dehydration salt solutions and drugs for diar-
with multiple drugs for diarrhoea prescribed in patent
rhoea by patent medicine dealers in Nigeria have been
reported by several authors.
5,6
medicine dealers shop, health centres and clinics, with
serious consequences. We describe here an illustrative
case.
Dear Editor, it is our contention that the intense cam-
paigns on diarrhoea prevention and management in
Infant BTO was admitted at eight months of age into the
childhood that were once mounted in Nigeria should be
Obio Cottage Hospital Oginigba, Port Harcourt, with
revisited. We may be beginning to lose the gains made.
history of diarrhoea, vomiting and fever for five days
and convulsions on the day of presentation. Child was
Thanks.
initially managed by patent medicine dealers with sev-
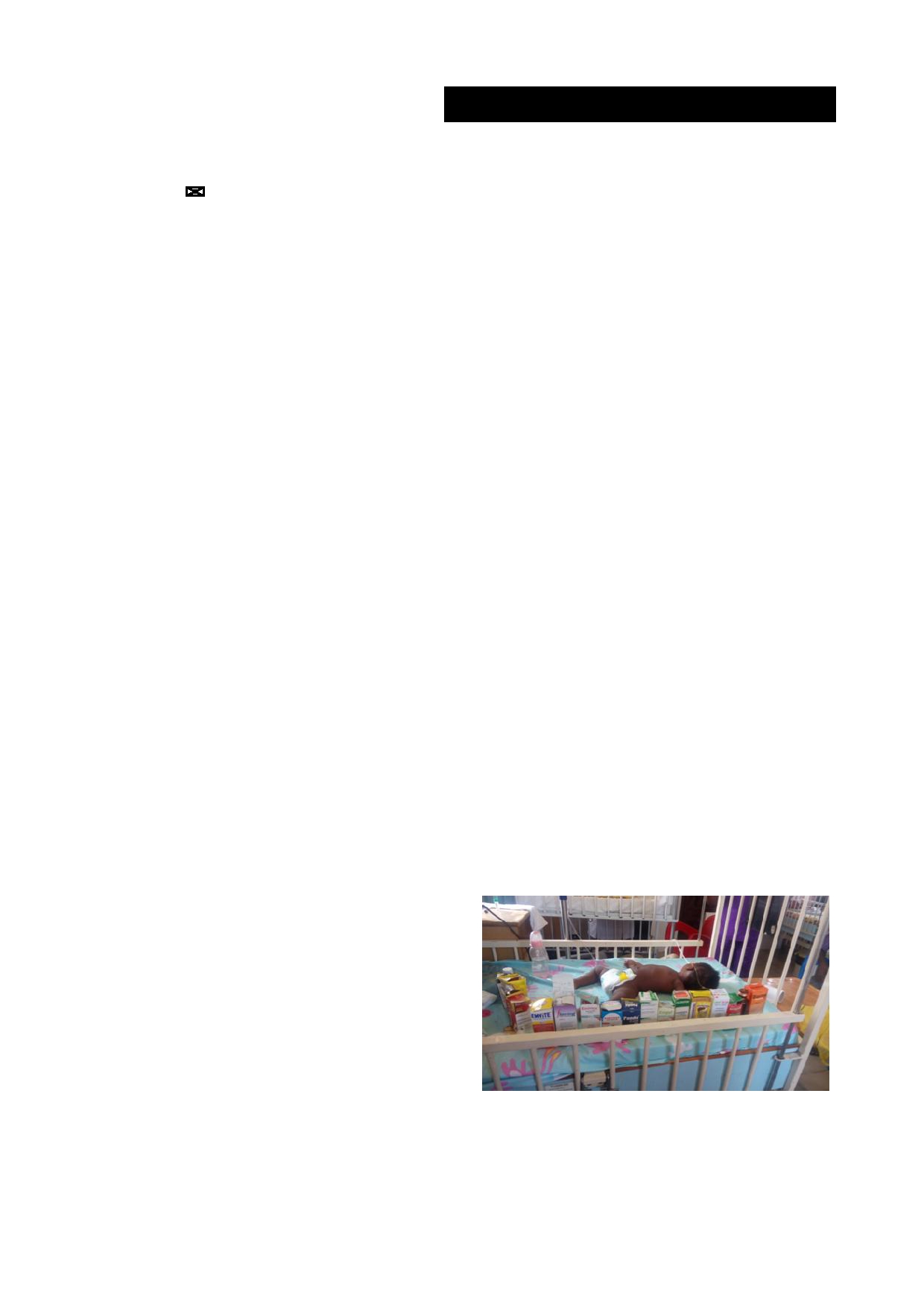
eral drugs as tabulated below Table 1 (see also fig 1).
Fig 1: 8
months old
infant with
feeding bottle
and some
of the
Standard ORS dissolved in 750ml of water was also
drugs given in the same episode of diarrhoea.
given. Child had fever (40.7 C), evidence of severe de-
o
hydration and seizures. Diagnoses of diarrhoea with
severe dehydration, hypovolaemic and septic shock,
bronchopneumonia (? aspiration pneumonia) and severe
malaria were made. PCV was 26%, sodium level
151mmol/l and random blood sugar 0.8mmol/l. Infant
was rehydrated with normal saline 20m/kg/hr repeated a
total of three times, seizures controlled with intravenous
diazepam. Intravenous ceftreaxone, and after urine pro-
duction, genticin were given. Hypoglycaemia was cor-
rected with ten percent glucose. After initial anti-shock
therapy, infant was given 75ml/kg of Ringers lactate
over six hours and then moved to ORS by naso-gastric

103
Table 1: Drugs
used/ abused
in the
index infant
Drug used/Abused
Usefulness in Diarrhoea
Adverse effects
Trade name
Active Substance
Anti-microbials
Emgyl
Metronidazole
Useful only in proven E. histo-
Diverts attention from ORS.
lytica and Gardia lamblia, both
Nausea
rare
in infants
Chloraphin
Chloramphenicol
Nil
against common diarrhoea
Can
cause bone marrow failure
organisms
Fleming
Amoxicillin + clavunalic acid
Not
effective against most diar-
Can
worsen diarrhoea
rhoea organisms. Useful in dysen-
tery (blood in stool)
Emmox
Amoxicillin
Not
effective against most diar-
Can
worsen diarrhoea
rhoea organisms. Useful in dysen-
tery (blood in stool)
Anti- Diarrhoeals/ Anti -Motility Drugs
Diastop
kaolin
No
proven use
Diverts attention from ORS.
Gives false impression of im-
Deshalom
kaolin
No
proven use
provement by thickening stools.
Rophelgan
Promethiazine
No
proven use
Drowsiness, sedation, extra-
pyramidal crisis which resembles
convulsions.
Poor appetite, child difficult to
assess accurately
CofN cold
Chlorpheniramide
No
proven use
Drowsiness, sedation, extra-
pyramidal crisis, dizziness, head-
Babyrex
Chlorpheniramine
No
proven use
ache, constipation,
blurring of vision, dry nose,
mouth and throat, irritability,
confusion, hallucination
Panda cold
Paracetamol
Pseudoephidrine can cause nau-
Chlorpheniramide
sea, vomiting, dizziness, head-
pseudoephidrine
ache, difficulty sleeping.
Colipan
Hyoscine bromide
Nil
Paralyses the intestine.
Abdominal distension which may
embarrass breathing
Maxiquine
Chloroquin +
No
proven use in diarrhoea.
Promethiazine effect,
Paracetamol + Promethiazine
Chloroquine not recommended
see
above. Chloroquin no longer
for
malaria
effective for malaria. Recently
banned by NAFDAC
Amodiaquin
Amodiaquin
Not
recommended alone for
malaria. No use in diarrhoea
References
1.
Liu
L, Johnson HL, Cousens S,
4.
Meremikwu M, Udoh E, Esu E,
6.
Aguwa E.N, Alebue P.N, Obi I.E.
Perin J, Scott S, Lawn JE et al ,
Chibuzor M, Effa E, Oduwole O,
Management of childhood diar-
Child Health Epidemiology Group of
et al .
Faclity-Based treatment of
rhoea by patent medicine vendors
WHO
and UNICEF, Global, regional
under-five diarrhoea in Cross
in
Enugu Local Government Area,
and
National causes of child mortality:
River State: A clinical audit.
Niger
South-East Nigeria. Int
J Med
Med
an
updated systemic analysis for 2010
with time trends since 2000.
Lancet
J Paed 2015; 31-18
Scs 2010; 2(3): 88-93
2012; 379 (9832): 2151-61
5.
Meremikwu M, Udoh E, Esu E,
7.
Uzochukwu BSC, Onwujekwe OE,
2.
WHO, the treatment of diarrhoea:
Chibuzor M, Effa E, Oduwole O,
Okwosa C, Ibe PO. Patent medi-
a
manual for physicians and other
et al .
Faclity-Based treatment of
cine dealers and irrational use of
senior health workers. Available at
under-five diarrhoea in Cross
medicines in children: the eco-
whqlibdoc.who.int>publications.
River State: A clinical audit.
Niger
nomic cost and implications for
Accessed 24-2-2016
J Paed 2015; 31-18
reducing childhood mortality in
3.
UNICEF/WHO. Readings on diar-
South East Nigeria. Plos ONE 9
rhoea student manual. Reproduced
(3): e91667.doi:10. 1371/
for
use in Nigeria by UNICEF
journal.Accessed 28-2-16
based on a document provided by
WHO. WHO/UNICEF