

Copyright 2015 © Nigerian Journal of Paediatrics. All Rights Reserved. . Powered by Pelrox Technologies Ltd
ISSN 03 02 4660 AN OFFICIAL JOURNAL OF THE PAEDIATRIC ASSOCIATION OF NIGERIA

|










Quick Navigation

Niger J Paediatr 2016; 43 (4): 264 268
ORIGINAL
Mohammed AA
Prevalence of rotavirus among
Aminu M
Ado
SA
children under five years of age
Jatau ED
with diarrhea in Kaduna State,
Esona
MD
Nigeria
DOI:http://dx.doi.org/10.4314/njp.v43i4.6
Accepted: 16th August 2016
Abstract :
Rotavirus (RV)
is a
(33.0%:63/111) compared to fe-
major etiological agent of acute
males (31.4%:66/210). The highest
Mohammed AA (
)
infantile gastroenteritis and is
burden was detected in children 25
Aminu M, Ado SA
associated with 20%-25% of diar-
-36 months of age (37.3%:22/59).
Jatau ED, Esona
MD
Department of Applied Science,
rhea
cases in infants. Nigeria con-
Highest prevalence was detected in
College of Science and Technology
tinues to be among the first five
children whose parents had pri-
Kaduna Polytechnic, Kaduna State,
countries with greatest number of
mary education (35.8%:19/53) and
Nigeria
RV
disease associated deaths per
those whose parents were civil
Email: aisha2zra@yahoo.com
year. The objective was to deter-
servants (35.6%:36/101). There
mine some demographic factors
was no statistically significant as-
that might be associated with rota-
sociation between breast feeding
virus diarrhea among children in
and RV infection (P> 0.05). The
Kaduna State. From September
study has revealed that rotavirus
2013-August 2014, 401 diarrheic
remains an important cause of
stool samples were collected from
acute diarrhea in children under
children under 5 years of age in
five years in Kaduna State, Nige-
Kaduna State, Nigeria and ana-
ria. Hence the need to introduce
lyzed for RV antigen using
the vaccines into the childhood
ELISA. An overall RV prevalence
immunization program in the
of
32.2% (129/401) was obtained
country
with
the infection
occurring
throughout the study period. The
Keywords :
Prevalence, Rotavirus,
infection was higher in males
Children, Kaduna State, Nigeria
Introduction
greatest number of RV disease associated deaths per
year. Estimates attribute up to 33,000 deaths annually to
RV
disease in Nigerian children less than 5 years old.
7,9
Diarrheal disease kills 1.8 million children under five
years of age yearly. It is the second leading cause of
1
Prevalence of 11.0%-56% have been reported in Nige-
ria.
5,12,13,14, 15,16,17,18,19,20
death, and accounted for 9.9% of the 6.9 million deaths
in
this age group in 2011. In Nigeria it is encountered
2
both in urban and rural areas. It is estimated that 1.3
3
The introduction of two effective RV vaccines (Rota
billion episodes and 4 million deaths occur each year in
Teq and Rotarix), licensed in 2006 and have been rec-
children under five years old with about 80% of deaths
ommended for use in all countries by WHO, particularly
occurring in the first two years of life.
4
in
those countries with high diarrhea-related mortality in
children younger than 5 years. Substantial declines in
21
Rotavirus (RV) gastroenteritis is a mild to severe dis-
ease, with incubation period of about 1-2 days. The
5
morbidity and mortality attributable to RV and all-cause
symptoms often starts with fever, nausea, and vomiting,
diarrhea have been recorded in high-income and middle-
followed by abdominal cramps and frequent watery diar-
income countries that have introduced RV vaccines so
far. Therefore, there is the need to introduce RV vac-
10
rhea, which may last for 3-8 days. Infected children may
also have a cough and runny nose.
5,6
Rotavirus infection
cine into the National Immunization Program.
is
more frequent in Africa, especially West Africa in-
cluding Nigeria in the cooler, drier winter months.
7,8
Rotavirus infection is not routinely diagnosed in most
Rotavirus is a major etiological agent for acute infantile
Nigerian hospitals probably due to the cost of its diagno-
gastroenteritis and is associated with 20%-25% of diar-
sis and because clinical spectrum of signs and symptoms
rhea cases in infants.
9,10
The number of deaths caused
are similar to other gastroenteritis. There is the need for
yearly by rotavirus has been estimated to be 453,000 in
regular detection of RV strains, because this information
children less than five years old annually worldwide.
11
is
needed to interpret the results of vaccine studies and
Nigeria continues to be among the 10 countries with
epidemiologic surveillance.

265
Rotavirus surveillance has been going on in Nigeria
Specimen Preparation
since 2010 at the Institute of Child Health,
University of Nigeria Teaching Hospital, Enugu.
20
Exactly 1 ml of sample diluent was added to properly
The aim of the study was therefore to determine the
marked tube using a pipette. For solid stool, the sample
prevalence of Rotavirus associated diarrhea among chil-
was pressed into transfer pipette to the first mark. For
dren under 5 years with diarrhea in Kaduna state
liquid stool, samples were aspirated into transfer pipette
Nigeria.
to
the first mark. Samples were re-suspended in 1 ml of
sample diluents. This makes a 10% fecal suspension.
Detection of Human Rotavirus
Materials and Methods
Study Area
Each
10% fecal suspension was screened for the pres-
ence
of rotavirus antigens using commercially available
The
study was carried out in Kaduna state, Nigeria. The
enzyme immunoassay (EIA) kit (Premier Rotaclone
state has a total number of 23 Local Government Areas
Meridian Bioscience, Inc. USA). All assays were per-
(LGAs) and three senatorial districts; that include south,
formed according to the manufacturers instructions.
north and central senatorial zones. Six of the LGAs were
The samples, microtiter wells and reagents were brought
selected by simple random sampling for this research.
to
room temperature before the test was carried out.
These LGAs include Kachia and Kagarko (south); Chi-
Wells for samples and controls were inserted into the
kun and Giwa (central) and Soba and Sabon gari (north).
microtiter well holder. About 2 drops (100µl) each of
The health care facilities selected were Primary Health
diluted fecal sample, positive control and negative con-
Care Unit (PHCU) Ladduga for Kachia LGA, PHCU
trol (sample diluents) was added to the bottom of sepa-
Buruku for Chikun LGA, PHCU Maigana for Soba
rate wells. About 2 drops (100µl) of enzyme conjugate
LGA, General Hospital Kagarko for Kagarko LGA,
was added to each well, mixed by gently swirling on
PHCU Gangara for Giwa LGA and Major Abdullahi
tabletop and was incubated at room temperature for 60 ±
Memorial
Hospital Sabon gari for Sabon gari LGA.
5
minutes. After incubation the liquid was poured out of
the wells into a discard vessel, and the microtiter well
Study Design
holder was tapped upside down vigorously against ab-
sorbent paper to ensure complete removal of liquid from
The research was a descriptive cross sectional study, and
the wells. All the wells were filled to overflow with
was conducted in a hospital or PHCU in each of the
washing buffer and the liquid was poured out. The mi-
LGA. Children under 5 years of age were studied. A
crotiter well holder was tapped upside down vigorously
diarrhea case was defined as a child passing 3 or more
against absorbent paper to ensure complete removal of
loose, liquid, watery stool in a 24 hour period.
liquid from the wells. The washing procedure was re-
peated two more times for a total of three washes.
Ethical Approval
About 2 drops (100µl) of substrate A solution was added
to
each well, and 2 drops (100µl) of substrate B solution
Ethical clearance was obtained from the ethical commit-
was added to each well, and it was incubated for 10 min-
tee of Kaduna state Ministry of Health.
utes at room temperature. Visual determination was
made after 10 minutes incubation. Samples with blue
Sample Size
color greater than negative control are taken to be posi-
tive, while samples showing equal or less color than
A
prevalence rate of 36.5% reported in a previous study
negative control are taken to be negative. Spectropho-
by
Wada-Kura
15
was used to calculate the sample size
tometric determination was done by adding 2 drops
using the equation by Sarmukaddam and Garad.
22
The
(100µl) of stop solution (Sulphuric acid) to each well
calculated sample size was 356.15. However to have a
after the incubation, and the absorbance of each well
good representation of the target population and to in-
was read at 450nm against an air blank within 60 min-
crease the chances of having positive samples, a total of
utes. Specimens with absorbance units (A
450 ) greater
401 diarrheic stool samples were used for the study.
than 0.150 were considered positive, while Specimens
with absorbance equal to or less than 0.150 are consid-
Sample Collection
ered negative.
A
total of 401 stool samples were collected from chil-
Analysis of Results
dren 0-5 years of age across the six selected LGAs.
About 5ml of fecal sample was scooped with a wooden
Data obtained from the questionnaire and the EIA was
spatula or decanted respectively into clean, labeled
analyzed using statistical package for the social sciences
screw capped tubes with the assistance of the laboratory
(SPSS) version 21. Chi-square and odds ratio was used
technologist. All samples were transported in ice box to
as
test of association and risk respectively at 95% confi-
the
Department of Microbiology, Faculty of Science,
dence interval with p ≤0.05 taken as statistically signifi-
Ahmadu
Bello University, Zaria and stored frozen at -
cant.
20
C until analyzed.
0
266
Results
The
result of the distribution of rotavirus with respect to
mode
of feeding is shown in Table 3. There was no
Out
of the 401 fecal samples screened for the presence
statistically significant difference between breast feeding
(
χ =3.124,df=1,
2
of
human rotavirus in children, 32.2% (129/401) were
and
the prevalence of rotavirus
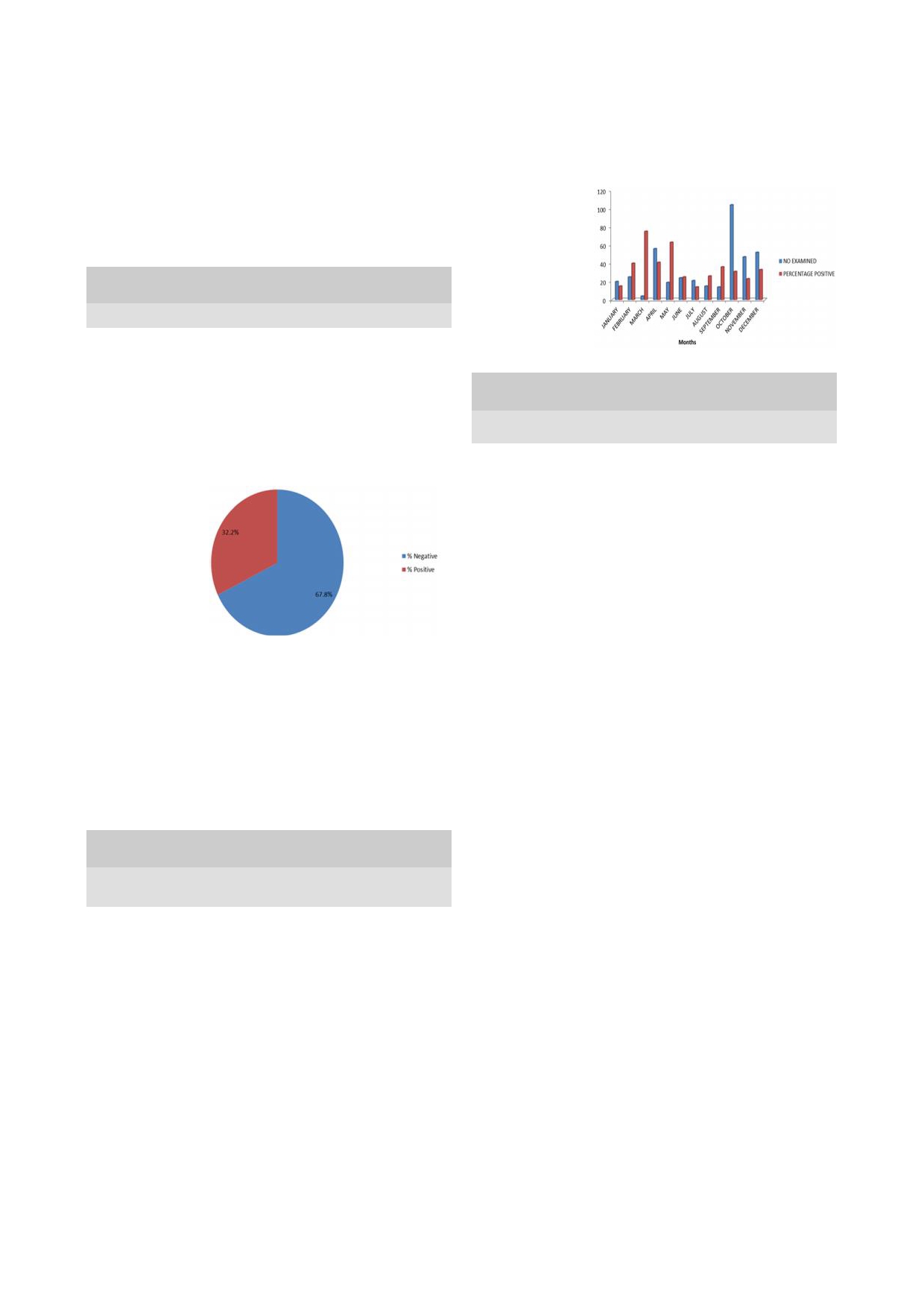
positive for rotavirus antigens (Figure 1).
p=0.562).
The distribution of rotavirus infection in children with
respect to location is shown in Table 1. There was statis-
Fig 2: Monthly
tically significant difference between prevalence of rota-
Distribution of
virus infection and location ( χ =13.651, df=5 p=0.031).
2
Rotavirus Among
Children in Kaduna
Table 1: Distribution
of Rotavirus
among Children
in Kaduna
State, Nigeria
State, Nigeria
Location (LGA) No examined No positive (%) No negative (%)
Chikun
58
21(36.2)
37(63.8)
Giwa
131
36(27.5)
95(72.5)
Kachia
41
25(61.0)
16(39.0)
Kagarko
62
14(22.6)
48(77.4)
Table 3: Prevalence
of Rotavirus
in Children
with Respect
to
Sabon gari
82
23(27.7)
60(72.3)
Breast Feeding and Introduction of Other Food
Soba
26
10(38.5)
16(61.5)
Mode of feeding Tested Positive Negative OR95% CI on ORp-value
Total
401
129(32.2)
272(67.8)
No
No
(%) No (%)
Breast feeding
( χ
=13.651, df=5, p= 0.031)
2
Yes
198
72(36.4) 126(63.6) 2.453 2. 500-2.732 0.562
No
203
57(28.1) 146(71.9)
Introduction of other food
Fig 1: Prevalence
Yes
328
100(30.5) 228(69.5) 3.1322.9 83-3.365 0.025
of
Rotavirus among
No
73
29(39.7) 44(60.3)
Children in Kaduna
State, Nigeria
Discussion
The monthly distribution of rotavirus infection in chil-
This study shows that rotavirus remains an important
dren in parts of Kaduna State was determined as shown
cause of infantile diarrhea in children. Rotavirus antigen
in
Figure 2. The highest prevalence was recorded in
was detected in children 0-5years in parts of Kaduna
March (75%:3/4), and least in July (14.0%:3/21)
state with a prevalence of 32.2% in this study. The result
(
χ =30.661, df=11, p=0.002).
2
is
similar to the 36.5% recorded in Kano Northern Nige-
ria
15
and 35.0% recorded in Lagos Southern Nigeria.
18
The result was analyzed according to some demographic
However the prevalence is higher than the 15.6% and
13
factors, and the result is shown in Table 2.There was no
previously reported in Zaria, the 11.0%
14
23.8%
16
statistically significant difference between sex, age and
and
13.8% reported in Jos, 18.0% in North-western Nige-
5
parents educational level and the presence of rotavirus
ria, 19.2% in Benin City and 56.0% in Enugu.
7
19
20
infection.
In
other African Countries, similar prevalence of 36.0%,
28.9% and 32.8% have been reported in Madagascar,
23
Table 2: Prevalence
of Human
Rotavirus in
Relation to
Demo-
Cote dvoire and Malawi respectively. In other parts
24
25
graphic Factors in Children in Parts of Kaduna State
Parameter Examined
Positive
Negative
p-value
of
the world, prevalence of 31.0% and 34.4% have been
reported in Bangladesh and Italy
26
27
No
No
(%)
No
(%)
Age group
(months)
The result however contradicts higher values of 57.4%
0-12
101
34(33.7)
67(66.3)
reported in Oman, 39.8% in Ghana, 45.5% in Ugan-
28
29
13-24
285
60(32.4)
125(67.6)
da
and 61.0% in Indonesia. Lower values of 14.0%,
30
31
10
25-36
59
22(37.3)
37(62.7)
0.039
[33]
26.4% and 26.2%
32
37-48
290
9(31.1)
20(68.9)
have been recorded in Namibia,
40-60
27
4(14.8)
23(85.2)
South Africa and Tunisia respectively.
Sex
Male
111
63(33.0)
128(67.0)
This observed difference in prevalence could be due to
Female
210
66(31.4)
144(68.6)
1.002
the method used, time and season of sample collection,
Parents educational level
sample storage, geographical location or environmental
Informal
170
51(30.0)
119(70.0)
factors. The hospital-based WHO global networks for
Primary
53
(35.8)
34(64.2)
Secondary 95
33(34.7)
62(65.3)
0.635
surveillance of rotavirus diarrhea report estimated the
Tertiary
83
26(31.3)
57(68.7)
rotavirus rate to range from 39-52% in the African re-
gion.
30
Parents occupation
The 32.2% obtained in this study, though high,
Self-employed 288
90(31.3)
98(68.7)
did not fall in this WHO African region range probably
Civil servant 101
36(35.6)
65(64.4)
0.043
because the sample were collected mainly from primary
Unemployed 12
3(25.0)
9(75.0)
health care units and not the main hospitals where seri-
ous cases are referred or taken to.
267
Rotavirus was detected in children throughout the study
cant
associated with the prevalence of rotavirus, this
agrees with the findings of Aminu
et al. and Junaid
et
12
period occurring with a slightly higher rate during the
al .
Children whose
parents had
primary education
had
5
dry
season. This agrees with the observation of previous
studies
7,8,10,15,23,25,34
who found the circulation of rotavi-
the highest prevalence while those whose parents had
rus lower during the wet season with slightly increased
informal education had the least.
seasonal peaks during the cooler, dryer months from
October to March. The higher prevalence of rotavirus
Children whose parents were unemployed had the least
infection in the dry season may be attributed to geo-
prevalence and civil servants had highest prevalence of
graphical and environmental factors with low relative
rotavirus, there exist statistically significant association.
humidity being the most important environmental fac-
This observation, could be due to chance and not a cer-
tor.
34
tainty, and this implies that rotavirus infect children re-
Rotavirus was recorded in all age groups in this study.
gardless of parents demographic characteristics.
Although highest prevalence was recorded among chil-
Breast feeding was not associated with the prevalence of
dren in age group 25-36 months, there was statistically
rotavirus in children. This contradicts the findings of
Aminu et
al.
35
significant difference between age and the prevalence of
who reported that breast feeding confer
rotavirus. This agrees with the findings of Wada-Kura
15
some protection against rotavirus infection. In this
who reported higher prevalence in children between 41-
study, children that were breast feed, and did not start
50
months in Kano and Coluchi et al . who recorded
35
any
food had higher prevalence; which could be due to
higher prevalence in children within age group 24-35
the
fact that at this age, children are more vulnerable to
months in Paraguay. The result however, contradict the
rotavirus infection. Breast feeding may only be protec-
36
report of Junaid et
al . and Aminu et
al .
5
in
studies
tive if it is practiced with intensity and frequency that
conducted in Jos and Zaria respectively, who reported
allows continuous high level protection of the intestinal
mucosa rather than sporadic or low volume feeds.
30
that the detection of rotavirus infection is more in chil-
dren under the age of two years. The higher prevalence
recorded in children among this age group (25-36
months) in this study could be due to behavioral activi-
ties of children at this age, who tend to play outside with
Conclusion
possibly fecally contaminated materials. Least preva-
lence was recorded in children above 40 months of age.
The study has revealed that rotavirus remains an impor-
This could be due to the fact that older children tend to
tant cause of acute diarrhea in children under five years
become protected from severe form of rotavirus infec-
in
Kaduna. There is the need for the introduction of the
tion as a result of protection acquired from multiple re-
licensed rotavirus vaccine in the study area as a means
infection.
13
of
preventing rotavirus infection.
Sex was found not to be associated with rotavirus diar-
rhea in children, this agrees with previous findings con-
Limitations
ducted in Nigeria.
12,13,15,16,34
Even
though in this study,
males had a slightly higher prevalence than females.
VP6
subgroup specificity could not be detected because
This
difference could be due to chance because at this
of
lack of monoclonal antibodies specific for VP6.
age there is no difference in life styles between the boy
and girl child. The result contradicts the finding of Jun-
aid et al . in Jos, who reported statistically
significant
5
Conflict of interest: None
association between sex and rotavirus infection.
Funding: None
Educational level of parents was not statistically signifi-
Reference
1.
World Health Organization,
4.
Sule EI, Aliyu AM, Addul-aziz
6.
Bass CW, Dorsey KN. Rotavi-
Estimated rotavirus deaths for
BM. Isolation of diarrheagenic
rus and other agents of viral
children under 5 years of age,
bacteria in children attending
gastroenteritis. In Nelson
2004, http;//www.who.int/
some selected hospitals within
Textbook of pediatrics, Edited
immunization monitoring/
Kaduna Metropolis, Kaduna
by
Richard E and Behrman F.
burden/rotavirus estimates.
State, Nigeria. Cont
J App
Sci
Raven press, Philadelphia;
2.
Fischer-walker CL, Rudan I,
2011,6 (1): 1 5.
2004: 107-110.
Liu L, Nair H, Theodoratov E.
5.
Junaid SA, Umeh C, Olabode
7.
Aminu M, Page NA, Ahmad
Global burden of childhood
AO, Banda, JM. Incidence of
AA, Umoh JU, Dewar J,
pneumonia and diarrhea. Lan-
rotavirus in children with gas-
Steele AD. Diversity of rota-
cet 2013, 381:1405-1416.
troenteritis attending Jos Uni-
virus VP7 and VP4 genotypes
3.
Adegunloye DU. Carrier rate of
versity Teaching Hospital, Ni-
in
Northwestern Nigeria. J
enteric bacteria with diarrhea in
geria. Virol
J 2011
8 (1):
233-
Infect Dis 2010, 202 (S1):198-
children and pupils in
238.
204.
Akure, Ondo State, Nigeria.
Acad J 2005, 4:3 6.

268
8.
Mwenda JM, Ntoto KM,
17.
Adah MI, Wade A, Tanguchi K.
28.
Albaqlani S, Peenze I, Dewar J,
Abebe A, Enweronu-laryea C,
molecular epidemiology of rotavi-
Al
lawah Z, Pearson L, Rupa V,
Ismail A, Mchomvu J, et al.
rus
in Nigeria: Detection of un-
et
al. Molecular characterization
Burden and epidemiology of
usual strains with G2P[6] and G8P
of
rotavirus strains circulating in
[1]
specificities. J
Clin Microbiol,
Oman in 2005. J
Infect Dis
2010,
rotavirus diarrhea in selected
2001, 39(11): 3969-3975.
202 (S1): 258-262.
African Countries: preliminary
18.
Audu R, Omilabu SA, Beer MD,
29.
Armah GE, Hoshino Y, Santos N,
results from the African rotavi-
Peenze I, Steele D. Diversity of
Binka F, Damanka S, Adjei R, et
rus surveillance network. J
human rotavirus VP6, VP7, and
al.
The global spread of rotavirus
Infect Dis 2010, 202 (S1):5-11.
VP4
in Lagos state, Nigeria. J
G10
strains: detection in Ghana-
9.
Parashar UD, Hummelman EG,
Health Popul Nutr 2002, 20 (1): 59
ian
children hospitalized with
Breese JS, Miller M.A, Glass
-64.
diarrhea. J
Infect Dis
2010, 202
RI. Global illness and death
19.
Iyoha O, Abiodun PO. Human
(S1): 231-238.
caused by rotavirus disease in
rotavirus genotypes causing acute
30.
Nakawesi J, Wobudeya E, Ndeezi
watery diarrhea among under-five
G,
Mworozi E, Tumwine JK.
children. Emerg
Infect Dis
children in Benin city, Nigeria.
Prevalence and factors associated
2003, 9:55-570.
Nig. J. Clin. Prac. 2015, 18: 48-
with rotavirus infection among
10. Page
N, Pager
C, Steele
AD.
51.
children admitted with acute diar-
Characterization of rotavirus
20.
Tagbo BN, Mwenda JM, Armah
rhea in Uganda. BMC
Peadiatr
strains detected in Windhoek,
G,
et al. Epidemiology of Rotavi-
2010, 10: 1-11.
Namibia during 1998-1999. J
rus
Diarrhea among Children
31.
Radji M, Putman SD, Malik A,
Infect Dis 2010, 202 (S1): 162-
Younger than 5 Years in Enugu,
Husrima R Listyaningsih E. Mo-
167.
South East Nigeria. Pediatr
Infec
lecular characterization of human
11. Tate
JE, Burton AH,
Boschi-Pinto
Dis J 2014, 33:S19-S22.
group A rotavirus from stool
C,
Steele, AD, Duque J, Parashar
21.
World Health Organization. Rota-
samples in young children with
UD.
2008 estimate of worldwide
virus vaccines: an update. Wkly
diarrhea in Indonesia. Sth
E Asi
J
rotavirus associated mortality in
Epidemiol Rec 2009, 84: 533-537
.
Trop Med Pub Health 2010, 41
children younger than 5 years be-
22.
Sarmukaddam SB, Garad SG. On
(2): 341-346.
fore the introduction of universal
Validity of Assumptions while
33.
Potgieter N, Beer MCD, Taylor
rotavirus vaccination programmes:
determining sample size. Ind J
MB,
Steele AD. Prevalence and
A
systematic review and meta-
Comm Med 2006, 29 (2): 2004
diversity
of rotavirus strains in
analysis, Lancet
Infect Dis
2012,
2006.
children with acute diarrhea from
12 (2): 136-141.
23.
Adiku TK, Dove W, Grosjean P,
rural communities in Limpopo
12.
Aminu M, Ahmad AA, Umoh, JU.
Comber P, Nakagomi T, Naka-
province South Africa from 1998
Rotavirus infection in four states in
gomi O, et al. Molecular charac-
to
2000. J
Infect Dis
2010, 202
North-western Nigeria. Nig
J Med
terization of rotavirus strains circu-
(S1): 148-157.
2008a, 17 (3): 258-290.
lating among children with acute
34.
Trabelsi A, Fodha I, Chouikha A,
13.
Pennap G, Umoh J. The prevalence
gastroenteritis in Madagascar dur-
Fredj
MBH, Mastouri M, Abde-
of
group A rotavirus infection and
ing
2004-2005. J
Infect Dis
2010,
laziz AB, et al. Rotavirus strain
some risk factors in pediatric diar-
202 (S1): 175-179.
diversity in the center coast of
rhea in Zaria, North Central Nige-
24.
Akran V, Peenze I, Akoua-Koffi
Tunisia from 2000 through 2003.
ria. Afr
J Microbiol
Res 2010,
4
C,
Kette H, De Beer MC, Steel
J Infect Dis 2010, 202 (S1): 252-
(14):1532-1536.
AD.
Molecular characterization
257.
14.
Nimzing L, Geyer A, Sebata T,
and
genotyphing of human rotavi-
35.
Aminu M, Esona MD, Geyer A,
deBeer M, Angyo I, Gomwalk NE,
rus
strains in Abidjan, Cote
Steele, AD. Epidemiology of
et
al. Epidemiology of adenovi-
divoire. J
Infect Dis
2010, 202
rotavirus and astrovirus infections
ruses and rotaviruses identified in
(S1): 220-30.
in
children in Northwestern Nige-
young children in Jos, Nigeria.
S
25.
Cunliffe NA, Ngwira BM, Dove
ria. Ann
Afr Med2008b,7
(4): 168
Afr J Epid. Infect 2000, 15: 40-42.
W,
Thinwa BDM, Turner MA,
-174.
15.
Wada-Kura A. Molecular charac-
Broadhead LR, et al. Epidemiol-
36.
Coluchi N, Munford V, Manzur J,
terization of rotaviruses detected in
ogy
of rotavirus infection in chil-
Vazquez C, Escobar M. Detec-
children under the age of five years
dren in Blantyre, Malawi 1997-
tion, subgroup specifity, and
with diarrhea in Kano State-
2007. J
Infect Dis
2010, 202
(S1):
genotype diversity of rotavirus
Nigeria 2011, An unpublished
S168-S174.
strain in children with acute diar-
M.Sc research thesis submitted to
26.
Bern C, Unicomb L, Gentsch JR,
rhea in Paraguay. J
Clin Micro-
the
school of postgraduate studies,
Banul N, Yunus M, Sack RB, et al.
biol 2002, 40 (4): 1709-1714 .
Ahmadu Bello University, Zaria.
Rotavirus diarrhea in Bangladesh
37.
Aminu M, Auwal G, Inabo HI,
16.
Gambo A. Prevalence of rotavirus
children: correlation of disease
Esona MD. Prevalence and effect
and
cryptosporidium pavum infec-
severity with serotypes. J
Clin
of
breast feeding practice on rota-
tions and their co-infection among
Microbiol 1992, 30 (12): 3234-
virus infection in children with
children with acute gastroenteritis
3238.
gastroenteritis in Zaria, Nigeria.
in
Zaria, Nigeria 2014, An unpub-
27.
Cascio A, Vizzi E, Alaimo C,
A
paper p resented at
the Elev-
lished M.sc research thesis submit-
Arista S. Rotavirus gastroenteritis
enth
International Rotavirus
ted
to the school of postgraduate
in
Italian children: can severity of
Symposium 3-5 September
studies, Ahmadu Bello University,
symptoms be related to the infect-
New Delhi India 2014, 164-
Zaria.
ing
virus? Clin
Infect Dis
2001, 32:
1126-1132.
165.