

Copyright 2015 © Nigerian Journal of Paediatrics. All Rights Reserved. . Powered by Pelrox Technologies Ltd
ISSN 03 02 4660 AN OFFICIAL JOURNAL OF THE PAEDIATRIC ASSOCIATION OF NIGERIA

|










Quick Navigation

Niger J Paediatr 2016; 43 (4): 246 251
ORIGINAL
Ndukwu C
Clinico - demographic factors
Onah S
Ebenebe J
associated with diarrhoeal disease
Osuorah D
outcome in under-five children:
A Nigerian tertiary hospital
experience
DOI:http://dx.doi.org/10.4314/njp.v43i4.3
Accepted: 4th August 2016
Abstract :
Objectives: To
deter-
period were aged below 5 years.
mine the proportion of under-5
Acute diarrheal disease accounted
Ndukwu C (
)
children presenting with diar-
for
32% and 38% respectively of
Onah S, Ebenebe J
rhoeal disease, and the clinico-
morbidity and mortality in these
Department of Paediatrics,
Nnamdi Azikiwe University
demographic variables associated
under-five children, with a case
Teaching Hospital, Nnewi.
with the outcome at the emer-
fatality rate of 18.3%. The mean
Email: ndukwu_ifey<@yahoo.com
gency paediatric ward (CHER) of
age at presentation was 11.96
the Nnamdi Azikiwe University
months with a male to female ratio
Osuorah D
Teaching Hospital, Nnewi, South-
of
1.4:1. Presentation with fast
Child Survival Unit,
East Nigeria.
breathing (Odds Ratio {OR} 2.6),
Medical Research Council UK,
Methods: Clinical
and demo-
convulsion (OR 2.5), loss of con-
the
Gambia unit, Gambia.
graphic details of patients with
sciousness (OR 4.3), increased
diarrhoeal disease as obtained
severity of dehydration, presence
from the Paediatrics emergency
of
one or more comorbidities (OR
ward log book over an 18month
4.68) and a co-diagnosis of sepsis
period were analyzed using SPSS
(OR 3.23) significantly affected
and Microsoft excel software
the outcome. (p< 0.05 in all these).
packages. The clinical variables
Educational status of the mothers
(non-parametric) were tested for
also significantly affected the out-
degree of association with mortal-
come. (F=9.08, p=0.023)
ity
using Spearmans rank correla-
Conclusion:
Intensified
effort
tion. Chi square and Fischer exact
should be made to sensitize the
test were used to determine pres-
public about dangers of inappro-
ence of significant differences
priate therapy and late hospital
between certain variables. A p
presentation of children with diar-
value <0.05 was deemed signifi-
rhoeal
disease. These will reduce
cant.
mortality-heralding complications.
Results: One
thousand, one
hun-
dred
and sixty three out of 1,513
Keywords: diarrhoeal
disease;
children admitted within the
mortality; sepsis
Introduction
ted through consumption of contaminated food and wa-
ter. Though there are effective interventions for diar-
2
Diarrhoea disease remains a leading cause of childhood
rhoea prevention like vaccines, promotion of early and
morbidity and mortality in developing countries like
exclusive breastfeeding, vitamin A supplementation,
Nigeria, and is presently described as one of the two
safe drinking water, improved sanitation; and safe effec-
biggest child killers globally.
1,2
It
trails only acute respi-
tive treatment protocols such as the use of low-
ratory infections in the under-five mortality toll, with
osmolarity oral rehydration salts (ORS) and zinc, chil-
about 1.5 million under-five children dying each year
dren are still dying because these interventions are either
from diarrhoea and about 80% of these deaths occurring
not available or accessible to the vulnerable, especially
in
the developing world.
2
in
Africa and South Asia; India and Nigeria, topping the
charts.
2,3
In
effect, diarrhoeal disease presently kills
When properly managed, the prognosis of diarrhoeal
more children than AIDS, malaria and measles com-
disease is excellent. Indeed, the mortality rate had im-
bined. In Nigeria, it accounts for 10% of morbidities
2,4
proved significantly over the last 40 years, following
amongst under- 5s.
5
global scaling up and widespread use of oral rehydration
therapy. Subsequently, with world attention diverted to
2
Diarrhoea has well defined risk factors and transmission
other global emergencies, there has been a decline over
routes with the inducing pathogens being often transmit-
the past two decades in the number of children accessing

247
recommended treatment for diarrhoeal disease in devel-
tre
at the extreme of severe dehydration with signs of
oping countries, with an upsurge in the number of un-
cardiovascular compromise and impaired organ perfu-
sion
are described as being in clinical shock. Available
9
treated or poorly treated children who present with a
spectrum of increasing severity of complications.
2,6,7
bed
side investigations include Rapid diagnostic test for
Region specific continuous evaluation of the burden and
malaria, urinalysis, random blood sugar. Side lab inves-
outcome of diarrhoeal disease is thus needful with high-
tigations include retroviral screening, packed cell vol-
lighting of the factors that impact on prognosis, as a
ume and films for malaria parasite. Urgent main lab in-
prerequisite to consolidate strategies that will reduce the
vestigations include full blood count, serum electrolytes
case fatality of this highly preventable and treatable dis-
and chest X-ray. The diagnosis of sepsis in the CHER is
ease.
based on signs of systemic inflammatory response like
tachycardia, tachypnea, abnormally high or low tem-
perature, leucocytosis and presence of presumed or con-
Methods
firmed infection. Data was entered in both SPSS version
16
and Microsoft Excel computer software packages.
This was a retrospective study carried out in the Chil-
Analysis was also done using these software packages.
dren Emergency Room (CHER) of the Nnamdi Azikiwe
Clinical variables were tested for degree of association
University Teaching Hospital, Nnewi. This is a Federal
with mortality using Spearmans rank correlation. Chi
Government owned tertiary and referral centre of excel-
square test was used to determine presence of significant
lence in Anambra state. This hospital receives referrals
differences between certain variables. A p value <0.05
from all around the state and some adjourning states like
was deemed significant. Relevant charts, tables and fig-
Delta and Enugu states. The CHER is manned by a full
ures were used to display frequency distributions of
retinue of staff running 2 shifts for doctors and 3 for
variables.
nurses. There are 2 consultant emergency paediatricians,
2
senior registrars during the morning shift and 1 senior
Study Results
registrar at night, a minimum of 1 resident doctor per
shift, 2 house officers during the day shift, 1 at night,
One thousand, five hundred and thirteen children were
and an average of 3 nurses in each of the nursing shifts.
admitted in the Children Emergency Room of the hospi-
The study population included all patients that were ad-
tal within the period. There were 872 males and 641
mitted in CHER from January 2013 to June 2014, with
females, with a male to female ratio of 1.4: 1. Children
acute diarrhoea. Those that were brought in dead and
under 5 years of age were 1163and constituted 77% of
those with diarrhoea that had lasted more than 2 weeks
all
the patients admitted. Three hundred and seventy two
were
excluded. Ethical approval to study morbidities
of
these U-5 children (214 males and 158 females) pre-
and mortalities in CHER within the time frame was ob-
sented with acute diarrheal disease giving a prevalence
tained from the Research and Ethical Committee of the
of
32%, with a male to female ratio of 1.4: 1. The mean
hospital. Data contained in a structured proforma was
age of these children was 11.96 months + 8.7. See Table
obtained from the doctors paediatrics emergency ward
1
below.
log
book. The CHER doctors log contains biodemo-
graphic
information on admitted patients as well as rele-
Table
1: age
and sex
distribution of
the patients
vant clinical details like symptoms, signs, diagnoses,
Age
(months)
Male N(%)
Female N(%)
Total
N(%)
investigation results, initial management and outcome in
1
11
125
(58.4)
97(61.4)
222(59.7)
the emergency room, as documented in the folders of
patients, retrieved after initial stabilization of the
12
35
80(37.4)
54(34.2)
134(36.0)
patients.
35
59
9(4.2)
7(4.4)
16(4.3)
Total
214(100)
158(100)
372(100)
Information extracted included the age, gender of pa-
Mean age is 11.96+ 8.7months, Median age is 10months
tients, birth order, parental occupation and highest edu-
cation level, presenting symptoms and duration of ill-
Other demographic characteristics:
Averagely the
ness, important signs, bedside and urgent initial investi-
socioeconomic class was middle class with up to 34% of
gations, diagnoses and outcome. Criteria for diagnosis
the patients being from the lowest social strata. Other
of
acute diarrhoea in the CHER is clinical, based on the
details are shown in table 2.
standard definition of an increase in daily stool fluidity,
frequency and volume from what is considered normal
Table 2: Demographic
characteristics of
patients
for an individual. This is made after a detailed history
2
Characteristics
Frequency (n = 372)
Percentage (%)
and thorough physical examination. The aetiological
Birth order
<4
322
86.6
diagnosis for diarrhoea was not included in the study.
>4
50
13.4
Diagnoses of morbidities like malaria, sepsis and bron-
Maternal age(years)*
chopneumonia are initially made clinically, but quickly
<35
298
80.2
followed up by bed side, side lab and urgent main labo-
>35
74
19.8
Maternal education
ratory investigations. The grading of severity of dehy-
Nil
formal
3
0.6
dration was based on the current World Health Organi-
Primary
60
16.2
zations clinically based criteria as no, some or severe
Secondary
191
51.3
dehydration. Routinely, children presenting in this cen-
8
Tertiary
118
31.8
*0.8%(3) of the mothers were teenagers aged between 18 and 19 years
248
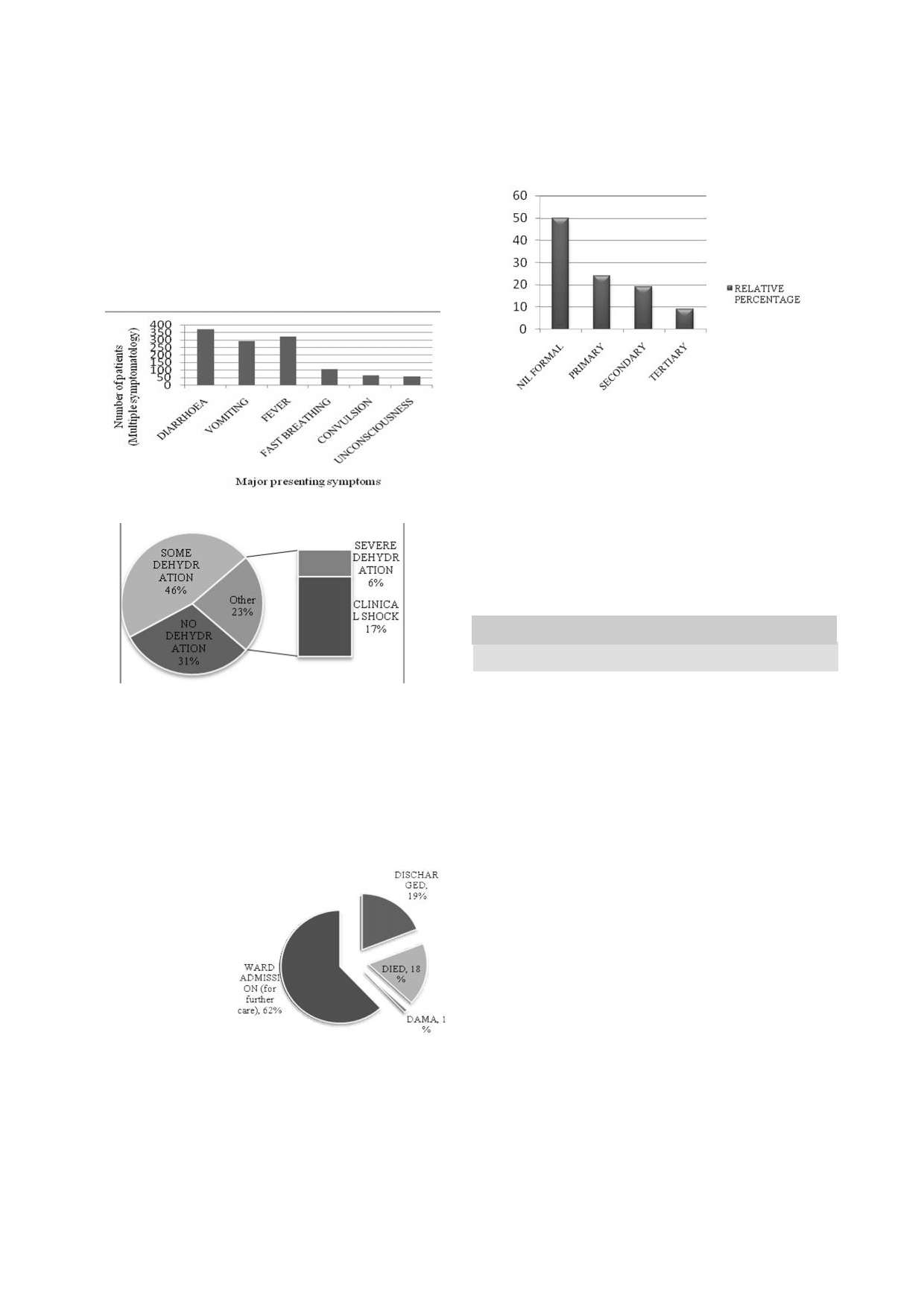
Clinical characteristics of the patients
: The
major
ciated with lower educational level. (F=9.08, p=0.023)
presenting symptoms of the patients are illustrated in
See Figure 4. Bivariate analysis was equally significant
Figure 1. Most (73.9%) of the patients presented within
at
0.01 level.
the first week of their initial symptom, while 8.3% pre-
sented after 2 weeks of initial symptom, other than diar-
Fig 4: Relative
percentage mortality per
educational level
rhoea (acute diarrhoeal disease occurred in these ones
secondarily). There was clinical dehydration at presenta-
tion in 68% (257) of them, with up to 25% of these be-
ing in clinical shock. Figure 2 is a representation of the
hydration state of the patients at presentation.
Fig 1: Major
presenting symptoms
of the
patients
Presenting complaints and outcome
Table 3 shows the cross-tabulation of presenting symp-
toms with the outcome of acute diarrhoea in the chil-
dren. Cconvulsions (OR 2.5, p<0.001), fast breathing
Fig 2: Levels
of dehydration
in the
patients
(OR 2.6, p <0.001) and unconsciousness (OR 4.3,
p<0.001) were significantly associated with fatal out-
come
in children with acute diarrheal disease. A signifi-
cant
strength of association with mortality in the patients
was also noted with these symptoms using bivariate
analysis.
Table 3: Association
of clinical
symptoms with
mortality
Symptom
Outcome
Odds ratio
p-value
(95% ci )
*
Mortality
Survived
Vomiting
54(18.4)
239(81.6)
1.0
0.885
Outcome of illness: Diarrhoea disease
was responsible
n=293(100)
(0.6-1.8)
Fever
58(18.1)
263(81.9)
0.9
0.792
for 38% of the 178 under-five mortalities recorded
n=321(100)
(0.5-1.7)
within the study period. Sixty eight of the372 children
Convulsion
**
24(36.4)
42(63.6)
2.5
0.000
with diarrheal disease died, translating to a case fatality
N=66(100)
(1.7- 3.9)
Fast breathing
***
rate of 18%. Up to 72% of these diarrhoeal related
35(32.4)
73(67.6)
2.6
0.000
deaths (49 of 68 patients) occurred within the first 24
n=108(100)
(1.7-3.9)
Unconscious-
30(51.7)
28(48.3)
4.3
0.000
hours of admission with many of them dying within
ness
****
(2.9-6.3)
minutes or few hours of presentation. The outcomes of
n=58(100)
the admissions are represented in Figure 3 below.
*
CI = confidence interval
**
Fig 3: Outcome
of
Spearmans correlation (0.217) significant at 0.005 level
***
diarrheal disease
Spearmans correlation (0.234) significant at 0.005 level
****
amongst under-fives
Spearmans correlation (0.372)significant at 0.005 level
Duration of illness and outcome : Effect
of duration
of
illness (time of onset of initial symptom) and duration of
diarrheal disease before presentation are represented on
table 4 below. The patients that presented earlier had a
significantlybetter outcome.
(F=10.69, p<0.05;X
2
=12.24, p<0.05)
Demographic characteristics and outcome:
Forty five
(65%) of the children that died were infants while the
rest were from 12 to 36months old. However this was
not significant. (F=4.475, p=0.10). The gender of the
patients also did not significantly affect the outcome.
(X
=2.69, p= 0.10)The only demographic characteristic
2
that had a significant relationship with the outcome was
maternal education with a higher relative mortality asso-

249
Table 4: Association
between the
duration of
illness, diarrheal
Discussion
disease duration and outcome
Duration of
Outcome
Statistic
p-value
This
study showed a high burden of diarrhoeal disease
illness
Mortality
Survived
morbidity and mortality amongst under-five year old
1-7
days
40(14.5)
235(85.5)
F=10.69
0.010
children that presented to the children emergency room
n=275(100%)
of
the Nnamdi Azikiwe University Teaching Hospital
8-14 days
21(31.8)
45(68.2)
n=66(100%)
within the study period, being responsible for about a
15
to 30 days
4(23.5)
13(76.5)
third of morbidities and mortalities amongst them. This,
n=17(100%)
alongside the high case fatality, confirms as has been
>30 days
3(21.4)
11(78.6)
documented in several studies and surveys both globally
n=14(100%)
and in Nigeria in recent years, that diarrhoea remains a
Duration of diarrheal disease
major cause of death in under-5 children.
1-4,10-3
In
the
X
=12.24
2
1
day
12(11.9)
89(88.1)
0.007
children emergency room of another tertiary hospital in
n=101(100%)
South East Nigeria, diarrhoeal disease was the common-
2
to 3 days
23(19.0)
98(81.0)
est
morbidity managed a year prior to this index study
n=121(100%)
and was responsible for 43% of all mortalities within the
4
to 7 days
18(16.5)
91(83.5)
period. A hospital based study in North central Nige-
11
n=109(100%)
8
to 14 days
15(36.6)
26(63.4)
ria, however, documented a far less prevalence (2.7%)
of
diarrhoea among under-5 children. The lower preva-
14
n=38(100%)
lence recorded in the study may be attributed to the lar-
F=
Fischers exact test
ger sampling frame which included all children admitted
X =
Chi square test
2
in
the Paediatric department of the tertiary Hospital over
a
period of 2 years unlike our study which enrolled only
Presence of dehydration, other co-morbidities and
outcome :
The level
of dehydration
of these
children at
under-5 children admitted into the emergency unit of the
the time of presentation significantly affected the out-
Paediatric department. Their prevalence was even lower
come. (F=89.43, p=0.000). Of all the patients who pre-
than the overall Nigerian prevalence of 10%, obtained in
sented in clinical shock, 63.5% died while 14.3% and
a
national survey in which the methodology involved
5.3% respectively, of all those that presented with severe
asking mothers about occurrence of diarrhoeal disease in
the two weeks preceding the survey. As diarrhoea tends
5
and some dehydration died. (See table 5) Presence of
one or more co-morbidities increased the odds of dying
to
be seasonal which was noted in the same survey,
from diarrheal disease. (OR 4.68, p=0.000). Children
these results would be largely dependent on the time of
who had sepsis at presentation to CHER were about
the survey.
three times more likely to die from acute diarrhoea than
those without sepsis on presentation (OR 3.23, p=0.000)
The outcome of diarrhoeal disease in this study was
(See Table 5). Bivariate analysis also showed a signifi-
worse in the children that presented with dehydration.
cant strength of association.
This is not surprising as young children are known to be
at
great risk of life threatening dehydration because of
Table 5: Dehydration,
co morbidities
and outcome
their high daily fluid turnover and decreased ability to
conserve water like adults, thus being unlikely to toler-
Level
of dehy-
Outcome
Statistic
p-value
ate increased loss of body water. The past gains of the
2
dration
Mortality
Survived
prevention of dehydration from diarrhoeal disease have
F
=89.43
*
No
16(13.9)
97(86.1)
0.000
not
been sustained, with studies documenting a de-
n=115(100)
creased awareness of the use and proper constitution of
Some
9(5.2)
164(94.8)
Oral Rehydration Salts (ORS).
2,12,15
n=171(100)
In
a 2010 study in
Severe
3(14.3)
18(85.7)
South East Nigeria, while 76% of the mothers knew they
n=21(100)
should use ORS for a child with diarrhoea, only 14.2%
Shock
40(63.5)
23(36.5)
of
them could correctly prepare ORS.
[15]
This decreased
n=63(100)
Co-morbidity
Odds ratio (CI)
awareness and knowledge will obviously negatively
One
or more
**
60(26.2)
169(73.8)
4.68
0.000
impact on the disease outcome and may be partly why
n=229
(2.31-9.5)
diarrhoeal mortalities are soaring. Even though the
Sepsis
***
33(39.3)
51(60.7)
3.23
0.000
mothers in our study were not questioned on their
n=84
(2.15-4.87)
PEM
8(28.6)
20(71.4)
1.64
0.143
knowledge of oral rehydration, the proportion of our
n=28
(0.87-3.07)
patients presenting with moderate and severe dehydra-
Malaria
9(18.8)
39(81.2)
1.03
0.928
tion and shock (over 68%), with significantly increasing
n=48
(0.55-1.94)
mortality based on severity of dehydration is highly sug-
Bronchopneu-
7(30.4)
16(69.6)
0.119
0.119
monia
(0.90-3.36)
gestive of ignorance on the caregivers part. Other re-
n=23
searchers have equally documented a strong and positive
correlation of a higher degree of dehydration to fatal
outcome in childhood diarrhoea.
16
*
Fischers exact test
**Spearmans correlation (0.259) significant at 0.005 level
***Spearmans correlation (0.294) significant at 0.005 level
Just
as found in our study, children with diarrhoea who
present to hospital with secondary symptoms like fast
250
breathing and unconsciousness have been equally docu-
procurement of drugs prescribed by patent medicine
dealers are initially exhausted.
6,12
mented in other studies to have increased odds for mor-
This might explain
tality. Known diarrhoeal complications such as electro-
3
why more than 2 out of every 10 of these index children
lyte imbalance, hypoglycaemia and dehydration result in
studied presented with severe dehydration, with most of
respiratory symptoms, seizures, altered consciousness
these being in shock. The functionality of the primary
and ultimately death. Apart from these secondary
16
and secondary health care in the region, where most of
symptoms, other conditions which are known causes of
the diarrhoea cases should have been initially managed,
mortality in children actually co-existed with the diar-
is
thus compromised as many of these children are hur-
rhoea disease in some of these children. This could ex-
riedly referred to the tertiary centre verbally, as experi-
plain the finding in this study of the presence of one or
enced in our centre, because of their critical condition.
more co morbidities being significantly associated with
mortality. Such findings have been documented previ-
ously.
3,12
Sepsis was the singular significant co-
morbidity that increased the likelihood of death from
Conclusion
diarrhoea disease in the study children. This is not sur-
prising as severe sepsis is a terminal event with a high
Diarrhoeal disease is still a major cause of under-five
fatal outcome in many infectious diseases, including
morbidity and mortality. The poor clinical state of many
diarrhoea in which clinical signs of severe sepsis with
of
the index patients at presentation was associated with
septic shock could overlap with hypovolemic shock.
3
poor outcome of illness. Delayed presentation to hospi-
tal until there are attendant co-morbidities and complica-
The significantly worse outcome seen in those with
tions such as severe dehydration, convulsions, fast
longer duration of illness has been documented in other
breathing and loss of consciousness were significantly
studies.
12,17,18
This
is expected because the longer lasting
associated with increase in the odds of death. Efforts to
a
diarrhoea episode is, and the longer it takes before
educate caregivers about timely rehydration and early
effective and appropriate care is sought for a child with
hospital presentation could reduce these mortality-
diarrhoeal disease, the more likely it is for serious and
heralding complications.
unsalvageable physiologic aberrations to set in. The
poor clinical state at presentation of a significant per-
centage of the children in our study could be an indirect
Authors Contributions
reflection of the health seeking attitude and literacy level
CN
and SO headed decision in diagnosis and manage-
of
the population studied. This is obvious and justified
ment of most of the patients. CN entered and analyzed
by
the fact that relatively, a higher percentage of chil-
the data. CN, SO and DO drafted the manuscript. CN,
dren of women with lower educational attainment died.
SO
and JE revised the manuscript.
Poorly educated women are less likely to indulge in safe
Conflict of interest: None
hygienic practices and may not recognise danger signs
Funding: None
in
ill children. It has been previously documented that
Nigerian children and children from other parts of Af-
rica are taken to health facilities when their illnesses are
considered severe with obvious failure of home and
Acknowledgements
other traditional therapy, contributing to late presenta-
tion to appropriate health facility.
6,12
With many of these
Drs Ofiaeli, Ngonadi, Nweke, Ameh, Azubuike and
parents influenced by cultural beliefs on the cause of and
Okafor, Paediatric residents in the emergency room at
treatment of diarrhoea, alternative options including
the time of the study for meticulous record keeping.
Reference
1.
Ban
Ki Moon Jonathan GE, Lake
3.
Mohammod JC, Monira S, Tah-
5.
National Population Commission
A,
Osotimehin B, Stoltenberg J,
meed A, Pradip KB, Hasan A,
(NPC)[Nigeria] and ICF Interna-
Radi A et al. The Global Cam-
Shafiqul AS et al. Progression of
tional. Nigeria Demographic and
paign for the Health Millenium
severe sepsis to septic shock in
Health Survey, 2013. Abuja, Ni-
Development Goals- Report 2013.
under-five diarrheal children in an
geria and Rockville, Maryland,
Accelerating Progress in saving the
urban critical care ward in Bangla-
USA: WPC and ICF Interna-
lives of Women and Children.
desh: Identifiable risks, blood iso-
tional. 2014.
Ministry of Foreign Affairs, Nor-
lates and outcome. Bangladesh
6.
Etea TD. Mothers perception and
way. January 2013. http://
Crit Care J. 2014: 2(1); 10-15
treatment seeking behaviour for
www.norad.no/globalcampaign et
4.
Centre for Disease Control and
childhood diarrhoea in Dendi
al.
Accelerating progress in saving
Prevention. Global water, sanita-
District, West Shoa, Ethiopia.
the
lives of women and children.
tion and hygiene. Global Diarrhoea
Glob J Med Pub Hlth 2014; 3 (3)
Global Campaign for the Health
Burden. US Department of Health
1-9
MDGs- Report 2013. United Na-
and
Human Services.
7.
Ene-Obong H, Iroegbu CU,
tions. 2013.
Uwaegbute AC. Perceived causes
2.
UNICEF/WHO. Diarrhea: Why
and
management of diarrhoea in
Children are Still Dying and What
young children by market women
can
be Done. New York: UNICEF/
in
Enugu state, Nigeria. J
Hlth Pop
WHO; 2009
Nutr 2000; (2)97-102

251
8.
World
Health Organization. The
11.
Anyanwu OU, Ezeanosike OB,
15.
Adimora GN, Ikefuna AN,
Treatment of Diarrhoea: A manual
Ezeonu CT. Pattern and outcome
Ilechukwu G. Home management
for
physicians and other senior
of
admissions at the children emer-
of
childhood diarrhoea: Need to
health workers. 2005 4 Revision
th
gency room at the Federal Teach-
intensify campaign. Niger
J Clin
WHO/CDD/SER/80.2. 6-7
ing
Hospital, Abakaliki. African J
Prac. 2011: 14(2) 237-41
9.
National Institute for Health and
Med Hlth Sciences. 2014.13(1)6-
16.
Stefano Guandalini and Carmen
Care Excellence. (NICE) Diar-
10 DOI: 10.4103/2384-
Cuffari. Diarrhoea disease. Med-
rhoea and vomiting in children:
5589.139435
scape 2014. Available from http://
Diarrhoea and vomiting caused by
12.
Blessing I., Abhulimhen-Iyoha,
emedicine.medscape.com/
gastroenteritis: diagnosis, assess-
Okposio M . Risk factors for
death
article/928598-overview. As-
ment and management in children
in
under-five children presenting
sessed 01/05/2015.
younger than 5 years. NICE clini-
with acute diarrhoea in an urban
17.
Lee WS, Boey CC. Chronic diar-
cal
guidelines April 2009. As-
teaching hospital in Nigeria.
Pa-
rhoea in infants and young chil-
sessed 21/6/15. http: //
cific J. Med Scie: 2013;12(1): 45-
dren: causes, clinical features and
publications.nice. org.uk/diarrhoea
52
outcome. Paediatr
Child Health.
-and-vomiting-in-children-cg84/
13.
UNICEF 2015. Monitoring the
1999 Jun;35(3):260-3.
notes-on-the-scope-of-the-
Situation of Children and Women.
18.
Ndukwu CI, Onah SK. Pattern
guidance.
Diarrhoea Disease. Available from
and
outcome of postneonatal
10.
UNICEF 2015. Monitoring the
http://data.unicef.org/child-health/
pediatric emergencies in Nnamdi
Situation of Children and Women.
diarrhoeal-disease. Assessed on
Azikiwe University Teaching
Diarrhoea Disease. Available from
01/05/2015.
Hospital, Nnewi, South East Ni-
http://data.unicef.org/child-health/
14.
Yilgwan CS, Okolo SN. Preva-
geria. Niger
J Clin
Prac 2015:
18
diarrhoeal-disease. Assessed on
lence of diarrhea disease and risk
(3) 348-53
01/05/2015.
factors in Jos University Teaching
Hospital, Nigeria. Ann
Afr Med.
2012;11(4):217-21.